
The Swirl Is Optional
We Replaced Six Meetings With 40 Minutes and a Chat Window. Healthcare Doesn’t Know This Is Possible.


VTE content directing anticoagulants in an order set should be straightforward. The content is well established. A pharmacist, a physician advisor, an informaticist, a couple rounds of edits, and it should be done. The reality is that even organizing the content was a process that swallowed hours and meetings, because the inputs arrived the way everything in healthcare operations arrives: scattered.
Guideline text is pasted from one source. A dosing spreadsheet is built in Excel by the pharmacist from multiple other sources. There was a screenshot of a different protocol that we wanted emulated and a reference table so mangled by whatever exported it that it is barely readable. Every input has its own format, speaks its own dialect, and has its own silo. Reconciling them into a single coherent structure is human work, or at least has been largely human work. In healthcare, human work means meetings and manually organizing. The cycle is familiar to anyone who has sat through it: collect the inputs, schedule the room, surface the disagreements, schedule the next room, wait.
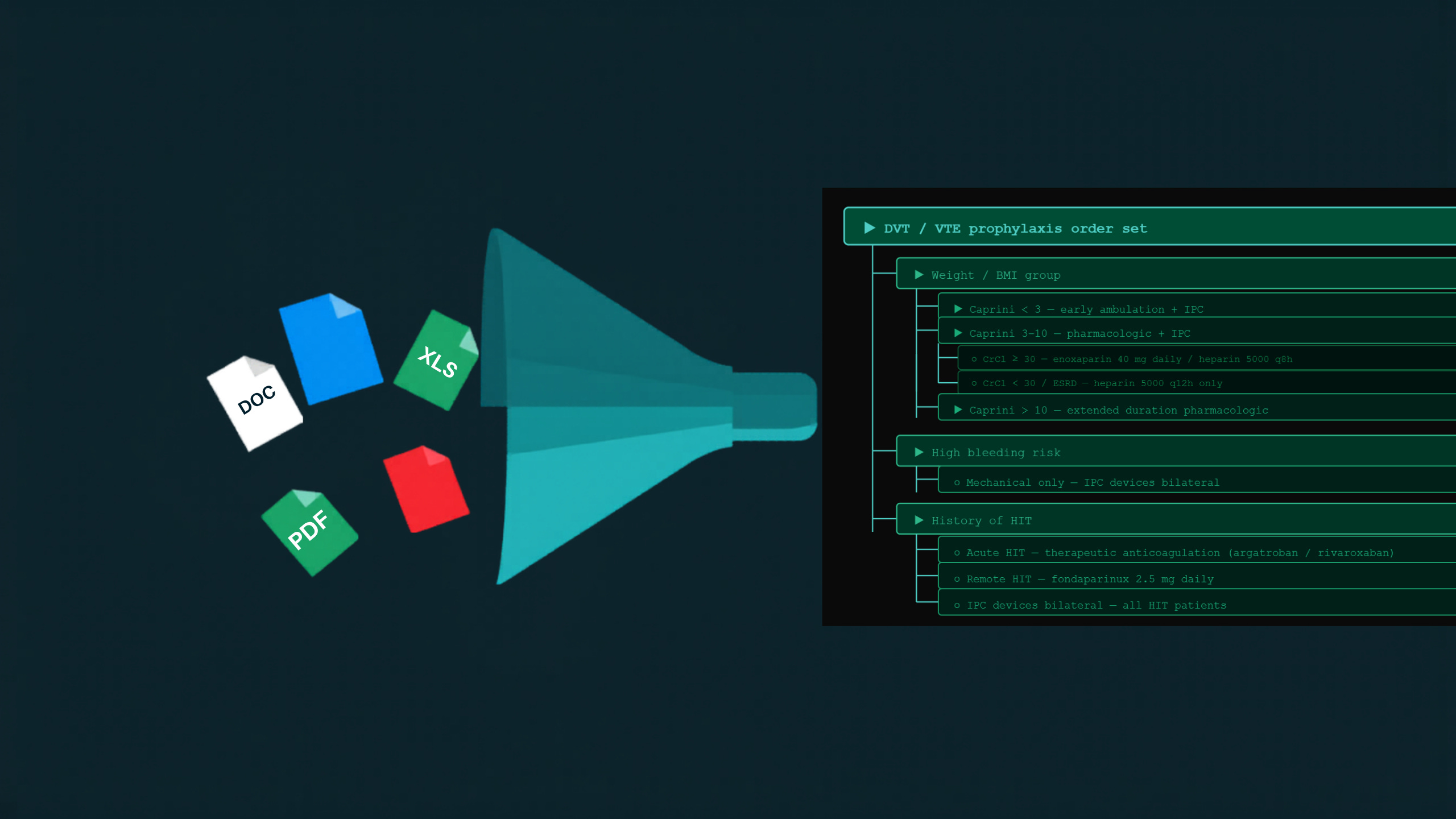
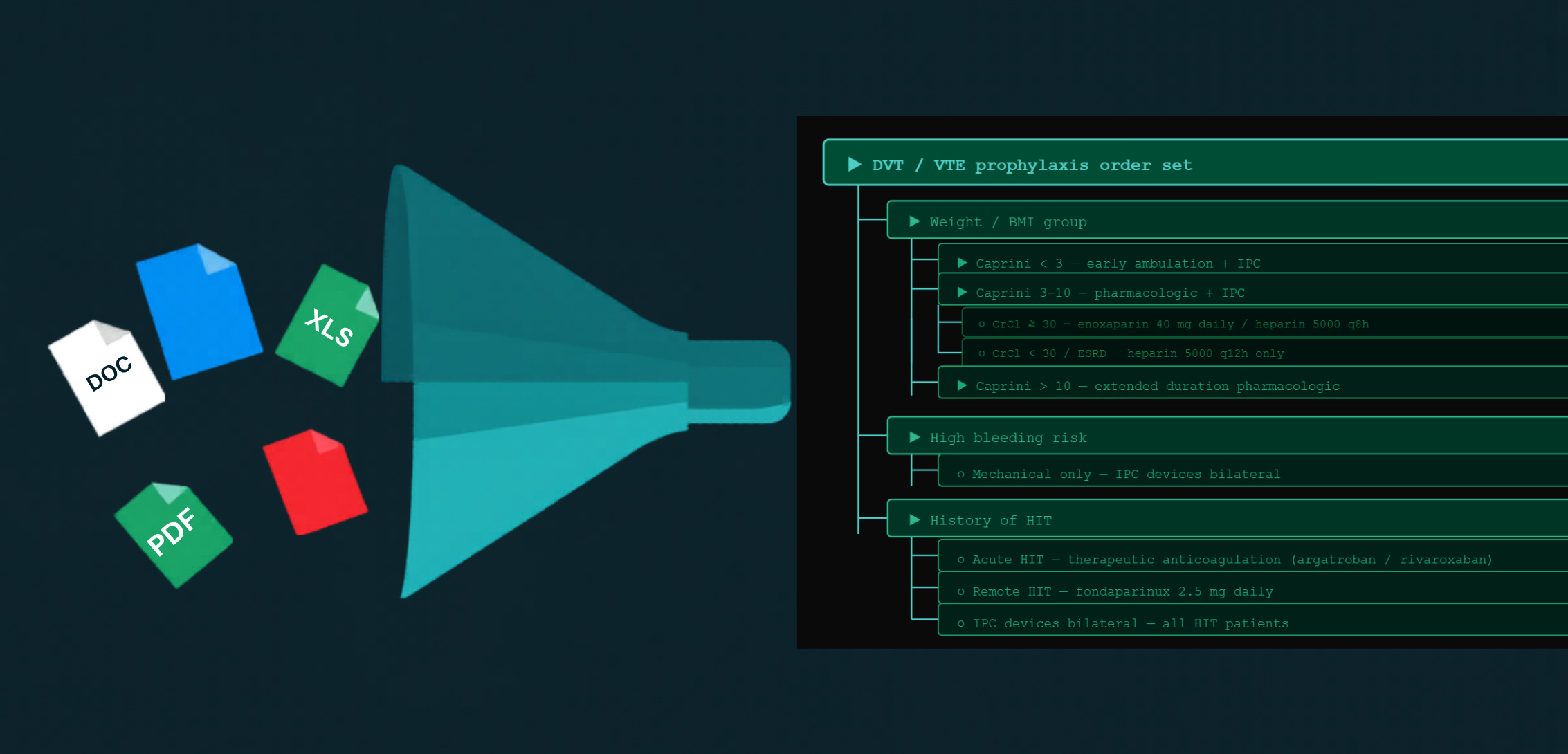
Last week a pharmacist and I did this differently. We opened an AI chat tool, pasted in the guideline text, attached the spreadsheet, dropped in the screenshot of the protocol she wanted the structure to emulate, and pasted the mangled table along with everything else. We gave the tool an example to emulate and guidance on what we wanted to end with: a nested order panel, risk-stratified, with carve-outs for renal impairment and for patients who can’t receive heparin at all. Then we iterated. We reordered the logic. We added the missing weight bands. Our initial version had sorting by risk score but then we realized that we wanted to sort by body habitus first, then risk score, then renal function. That particular edit took about thirty seconds. In previous iterations it would taken at least half an hour of rearranging and editing. All told, we spent about forty minutes doing this and then we had a clean, architected order set structure she could use as a blueprint to build.
The tool did not build the order set. It never touched Epic. It produced the architecture, the decision logic, the nested structure, in a very readable form that made her order set build easy. The build still happens in the system, but we removed hours and days of swirl.
The Unlock Is Not the Agent. It Is the Mess You Already Have.
The AI conversation in healthcare is dominated by the impressive layer. We are inundated by shiny objects: agents that act on their own; bots that triage; vibe coding that spins an app out of a sentence. These are real, and each one solves a real problem. But they all are still difficult to access for mere humans. There aren’t hordes of vibe coding Epic application analysts out there. But there are tools available to almost anyone who deals with swirl. In our system, that is almost everyone.
The most accessible thing is the chat window people already keep open and use as a better search engine. It is available to anyone with a browser. You do not have to clean your inputs before you hand them over. You can give it the pile exactly as the pile exists then iterate.
After all, who in healthcare operations does not have large volumes of disorganized inputs? Spreadsheets, PDFs of records, Word files, email threads that contain the one decision everyone half-remembers. A tool that turns that pile into a structured first draft is not a niche capability for the technically adventurous. It is the most broadly applicable thing in the room, and it is sitting in a tab that everyone already has access to that most people are using to look up the latest GLP-1 indications or the weather on the drive home.
What We Actually Pay For Is the Swirl
The expensive part of operational healthcare work has never been the final product. It was the cognition and convergence before the final product: the meetings to gather the inputs, the meetings to reconcile them, the version that goes around for comment, the data collection, the waiting between rounds. The order set itself is at most a few hours of build. The swirl in front of it is what turns a few hours into a few weeks consuming multiple stakeholders’ time.
The forty minutes with two people felt good because of what we accomplished. What felt better was that we didn’t have to spend two more weeks and six more meetings to finalize the content. The rounds of human reconciliation never had to happen because the structure arrived legible the first time. It is a small example, but it is emblematic of many other examples that are waiting for us to leverage.
This approach applies not only to clinical content. It applies to a project charter, a requirements document, a go-to-market plan, any operational work whose first hard step is making scattered context coherent. Healthcare runs on that step constantly and almost never counts the grind as an avoidable cost. We treat the grind as the weather. It is something we just need to live with. It is not the weather. It is a process we built, and it is now the part that can be the easiest to fix.
We Keep Replacing the Power Plant
Erik Brynjolfsson tells the story of what happened when American factories electrified. I have used the example many times because the metaphor is so apt. The first productivity gains from electricity were small, because factory owners did the obvious thing. They pulled out the steam engine and bolted in an electric motor, and changed nothing else. The floor was still laid out around a single enormous central drive shaft, machines crowded near the power source, because that is how a steam factory had to work. The real gains came decades later, when someone redesigned the floor around what electricity made possible. Distributed motors. Machines placed by the logic of the workflow instead of by proximity to the shaft. The power source was the easy substitution. The redesign was the unlock.
Healthcare is at the bolt-in-the-motor stage. We drop a chat tool into the existing process and ask it to speed up one step inside a workflow we have not touched. That helps, and it is worth doing. But the structural gain only shows up when we redesign the process around the fact that synthesis is now cheap. If turning chaos into a structured draft takes forty minutes instead of a week, then the committee cadence built around the week-long version is now the bottleneck. The synthesis stopped being the constraint. Almost nobody is redesigning the committee. We are admiring a fancier motor mounted to the old floor.
I should be honest about my approach, because this example describes my own M.O. For years, my instinct has been to work at the level where I have direct influence. The configuration I can do myself. The single analyst I have a relationship with, where a quiet conversation and a good example move a build forward without anyone needing executive sign-off. That is where I am effective and it is where I am comfortable. A session like the pharmacist’s is satisfying to me for exactly that reason. It proves the point, it lights a lightbulb in the room, and then I move on to the next one. I am a physician builder, but building isn’t the same thing as changing.
That is water flowing around the boulder. I have written before about water finding the crack, adjusting to the object, making its way through rather than against it. It is an effective way to survive inside institutions that resist change. It is a difficult way to move the boulder. Getting the dopamine hit from a clean demo preserves the relationship and the project, and it leaves the factory floor exactly as it was. The redesign I keep describing is the conversation I have difficulty executing. It isn’t the discussion with the factory workers. It is the discussion with the people who actually own the floor.
The Easy Part and the Hard Part Got Swapped
The technology is not the hard part. That is the insight the pharmacist’s forty minutes demonstrated. The capability is accessible, ubiquitous, and sitting in a tab. Feeding it the mess is the most natural thing in the world, because the mess is what we all already have.
The hard part is the redesign. The will to treat “how we convene, gather, and decide” as something to rebuild rather than preserve. The executive who looks at a forty-minute result and asks not “can we use this tool” but “what is our process still optimized for, and why.” We have been treating the technology as the obstacle and unlock because the technology lets us avoid the obstacle that is actually us. The unlock is really the redesign.
A single trickle finds the crack. Enough of them together become the torrent that moves the rock. I am writing this to find out who else is already in the water.
John Lee is an emergency physician and Epic consultant who helps health systems bridge the gap between Epic’s capabilities and operational reality. He specializes in data architecture, registry optimization, and making Epic’s tools actually deliver results.
If you need help configuring your Epic environment to support these capabilities, connect with him on LinkedIn or via his website.